.jpg) |
| Ref: https://www.runwell.net.au/blog/ |
Foam roll massage and tennis ball massage is a popular technique of muscle - fascia tension release for prevent and treatment benefits. It is applied to many parts of the body and musculoskeletal impairments including the IT band syndrome.
In my physiotherapy clinic experience with IT band syndrome patients, I have used this technique many times that roll on the IT band directly as the standard management. The outcomes demonstrated both effectiveness and ineffectiveness. Finally, I found a way to massage with the foam that I always recommend to patients who are with IT band syndrome.
 |
| Ref: https://physioworks.com.au/pain-injury/knee-pain/itb-friction-syndrome/ |
I have seen muscle spasm not only at mid IT band but also above knee cap, rear hip joint, calf muscles.
5 ways to do roll massage in IT band syndrome
Exercise #1: IT band: lying on the side to roll.
Exercise #2: Gluteus maximus: it is necessary to bend hip joint with half - prone in front.
Exercise #3: Tensor Fascia Lata: prone on the ball to roll.
Exercise #4: Biceps femoris: lying on the side with half - supine.
Exercise #5: Vastus lateralis: lying on the side with half - prone.
I would like to introduce all muscles anatomy which I have recommended to do foam roll; include,
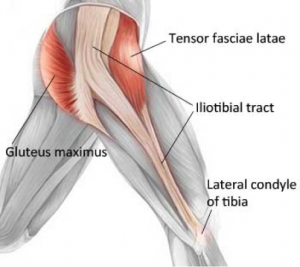
(1) The IT band
IT band is a strong thick wide tendinous band located on the lateral thigh. IT band origin is insertion attachment of gluteus maximus (Gmax) and Tensor Fascia Latae (TFL) that extend their part into the IT band directly. The mass of the IT band descended along the lateral thigh to the knee joint that covers the vastus lateralis muscle. The IT band has 2 primary attachments, including the lateral epicondyle and the Gerdy tubercle.
 |
| Ref: https://www.mygcphysio.com.au/ |
The first iliotibial band attachment is into the distal femur at the upper edge of the lateral epicondyle. The histologic makeup is consistent with tendon and has a layer of adipose tissue underneath the iliotibial band attachment area. The adipose tissue contains pacinian corpuscles, is highly vascular, and may be “the site of the inflammation” that causes pain during compression.
The second attachment of the iliotibial band is the insertion into the Gerdy tubercle of the tibia and serves as a ligament in structure and function. The Gerdy tubercle attachment is tensed during tibia internal rotation as the knee flexes during the weight-acceptance phase of gait. Internal tibial rotation explains the occasional connection between toeing in and iliotibial band “strain”
Moreover, there are many distal attachments that span out to the lateral border of the patella (by way of epicondylopatellar ligament and patellar retinaculum), patellar tendon, lateral patellar retinaculum before its insertion on Gerdy’s tubercle of the tibia, the biceps femoris, and vastus lateralis.
About this muscle, I have seen trigger points at mid IT band and 2 - 5 cm. above knee joint the most.
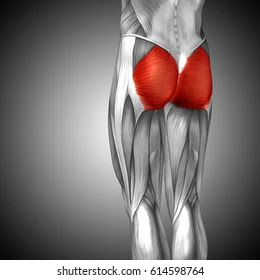
(2) Gluteus maximus (Gmax)
We can see Gmax at the rear hip which is the biggest muscle that is why origin attachment of Gmax covered large area; include, posterior ilium, posterior layer of thoracolumbar fascia, posterior superior iliac spine (PSIS), posterior gluteal line, posteroinferior sacrum, coccyx, sacrotuberous ligament, and over on gluteal fascia. It is used for support and bumpers while sitting in our daily lives. Gmax has two distinct portions that consist of inserts into the IT band and the inferior portion inserts into the femur. The Gmax pulls posteriorly on the IT band and femur to extend the hip.
According to its insertion, there is thickening and stiff soft tissue behind the greater trochanter.
(3)Tensor Fascia Lata (TFL)
Origin of TFL started on anterolateral of an iliac crest that is approximately 15 - 76 millimeters wide. TFL has many origin attachments; include, the lateral aspect of the anterior superior iliac spine (ASIS). The iliac tubercle, a notch located below the superior spine of the ilium, the anterolateral iliac fossa that is slightly below the crest, and the deep surface of the fascia lata of the thigh.
Insertion of TFL has been recorded in many locations. There are disputes , for example, on greater trochanter or around there, to the middle layer of the IT band. So, It is not clear whether such tendinous tissue belongs to the fascia lata, or is the muscle’s own tendon. However, the TFL pulls anterosuperiorly on the ITB to flex the hip generally.
I have found tightness, stiffness, and trigger points on this muscle often that related IT band tension progressively.
 |
| Ref: https://www.pinterest.com/pin/ |
(4) Biceps femoris
Biceps femoris is a member of the hamstring muscle which is located on the lateral side of the posterior thigh. They consist of long head and short head that short head originated medial to the linea aspera of the distal femur and descended distally and laterally.
The first component of the short head was a proximal muscular attachment to the anterior and medial side of the tendon of the long head. Other significant insertions included an attachment of the capsular arm to the posterolateral joint capsule, the attachment of the capsuloosseous layer to the iliotibial tract (biceps-capsuloosseous iliotibial tract confluens), a lateral aponeurosis, two tendinous attachments-the direct arm, the anterior arm, and capsular attachment in the interval between the tendon of the lateral head of the gastrocnemius. Perhaps, insertion anatomy caused patients with IT band syndrome to feel tense calf muscle.
My own opinion, it is not clear between biceps femoris tightness or posterior fiber of IT band stiffness.
 |
| Ref: https://anatomy.app/encyclopedia/biceps-femoris |
(5) Vastus lateralis (VL)
VL is a member of quadriceps composed structurally of four distinct muscles; include, the rectus femoris, vastus lateralis, vastus medialis and vastus intermedius. The vastus lateralis is considered the largest part of the quadriceps femoris to form thick, wide and fusiform appearance is intimately attached to the vastus intermedius in its middle third.
The origin of the vastus lateralis is on the greater trochanter, lateral lip of linea aspera femoris and the lateral intermuscular septum and its insertion at the base patellar ligament using the patella and tibial tuberosity.
Vastus lateralis muscle has presented two parts; include, long and oblique parts. The oblique portion arises from the linea aspera of the femur and lateral intermuscular septum, a more fibrous expansion of the iliotibial tract by inserting the tendon itself, which is directed inferior and lateral to the vastus lateralis muscle over this by joining the superolateral border of the patella tendon to form a single, often attached to the joint capsule. The distal fibers of the vastus lateralis oblique were presented in interdigitated lateral retinaculum, which is formed from the expansions of tendinous insertions of the vastus lateralis muscle, inserted in the tibia and patella which, in turn, reinforces the anterolateral region of knee, and iliotibial tract. Morphologically, the vastus lateralis oblique is divided into: a distal surface and a spiral proximal portion with deep longitudinal fibers in the femoral shaft below the belly of the vastus lateralis muscle along, mingling with the vastus intermedius.
 |
| Ref: https://learnmuscles.com/glossary/vastus-lateralis/ |
The vastus lateralis longus has its origin in the femoral trochanter and lateral lip of linea aspera of the femur, as found in the anatomical literature. showing extensive superficial aponeurosis in more than two thirds of the proximal surface and a deep aponeurosis in the distal 1/3 separating it from the vastus lateralis obliquus. Its insertion is on the superolateral border of the patella by the patellar ligament by means of union with the tendon of vastus lateralis oblique, forming a single tendon.
Therefore, the extensive lateral oblique is clouded by the IT band giving rise to the lateral retinaculum and completely covering the vastus lateralis oblique.
 |
Bridging kneeout to strength glut
(Ref: https://www.skimble.com/) |
Finally, I would like to recommend you to make rolling massage combine strengthening glut muscles that is very important and stretching that follow on https://yimphysionearme.blogspot.com/2022/05/physiotherapy-with-6-optionals-tfl-itb.html
Reference:
https://www.researchgate.net/publication/51211560_Iliotibial_Band_Syndrome_Soft_Tissue_and_Biomechanical_Factors_in_Evaluation_and_Treatment/link/59dce6f8458515e59df9eeca/download
https://link.springer.com/content/pdf/10.1007/s40279-021-01634-3.pdf
https://www.scielo.br/j/rbme/a/htP9y5rrfQdkGFLDkZPQF6r/?lang=en&format=pdf
http://www.jms.periodikos.com.br/article/587cb49f7f8c9d0d058b47a1/pdf/jms-28-4-587cb49f7f8c9d0d058b47a1.pdf
https://www.researchgate.net/publication/14561312_The_Biceps_Femoris_Muscle_Complex_at_the_Knee/link/5421e5de0cf2a39f4af766e9/download
https://www.researchgate.net/publication/51823221_A_review_of_the_anatomy_of_the_hip_abductor_muscles_gluteus_medius_gluteus_minimus_and_tensor_fascia_lata





.jpg)










.jpg)



